
Pulmonary valve stenosis (balloon valvuloplasty)
Pulmonary valve stenosis occurs both as a single malformation and as part of complex heart defects.
Treatment of pulmonary valve stenosis in children is almost always catheter-interventional. Only if the valve is too small overall and severely malformed will the surgeon selectively incise the narrowed parts of the valve (commissures) and expand the valve annulus (retaining apparatus). In this case, balloon valvuloplasty is usually not successful.
Indication
Pulmonary valve stenosis is indicated for treatment if the pressure load on the right ventricle is too high, but also if the child is markedly cyanotic and the right ventricle is hypoplastic. The following threshold values and indications correspond to international guidelines:
- Critical pulmonary stenosis of the newborn
- Severe pulmonary stenosis with symptoms
- Doppler gradient on ultrasound ≥ 50 mmHg (infant)
- Doppler gradient on ultrasound > 40 mmHg (schoolchild, adolescent)
Simultaneous leaks that are more than second degree no longer permit balloon valvuloplasty.
Technics
Balloon dilatation is safe to perform with today's technology and has a very low mortality rate (0-0.5%), even in newborns.
A catheter is manoeuvred into the right ventricle via the inguinal vein (femoral vein) and from there into the pulmonary artery. The actual balloon catheter can then be positioned in the valve via a guide wire. The procedure is based on the balloon slightly tearing the adhered pocket valves. The diameter of the balloon in relation to the diameter of the pulmonary valve is always selected to be approximately the same size or up to 1.5 times larger.
Course
Many patients with pulmonary valve stenosis can be treated with a single balloon dilatation. However, this only applies to valves that are not severely malformed. In this case, catheter intervention helps to prolong the time until surgical treatment.
Dilatation of a pulmonary valve stenosis
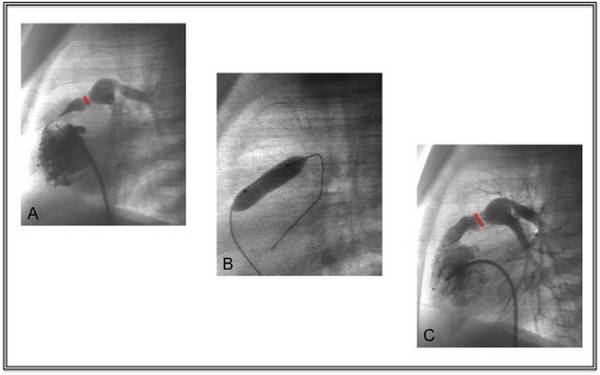
A Illustration of the severe narrowing of the pulmonary valve (red marker),
B Position of the balloon in the valve,
C Result of the dilation with the valve region now clearly widened.